

A 19-year-old man is evaluated after being stabbed in the back. Vital signs are normal. Neurologic examination demonstrates the absence of motor activity in all muscle groups of the right lower extremity, as well as decreased muscle tone. Left leg motor function is normal. Right patellar reflex, Achilles reflex, and Babinski sign are absent. There is loss of light touch and proprioception below the right costal margin. Pinprick sensation is absent on the left side at the level of the umbilicus and below. Which of the following is the most likely location of this patient's injury?
Below is the code for an example image modal link
Flashcards
{kind=link}
/* -- Un-comment the code below to show all parts of question -- */
| A. Complete spinal transection at T10 | ||
| B. Left spinal hemisection at T8 | ||
| C. Left spinal hemisection at T10 | ||
| D. Right spinal hemisection at T8 | ||
| E. Right spinal hemisection at T10 |
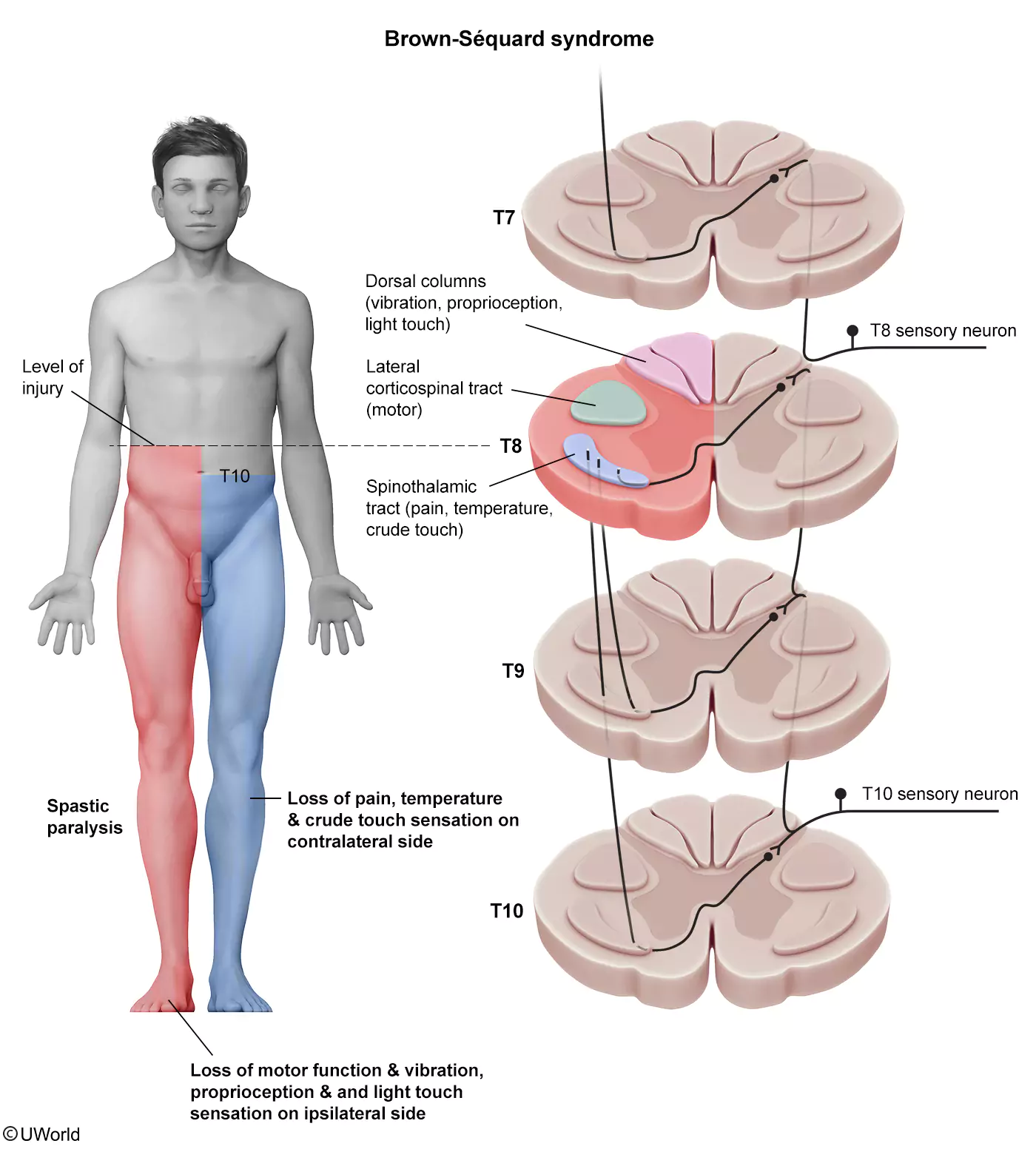
This patient who was stabbed in the back has a variety of neurologic deficits concerning for Brown-Séquard syndrome. This syndrome typically occurs due to hemisection (ie, disruption to half) of the spinal cord. Findings include the following:
- Ipsilateral hemiparesis: lateral corticospinal tract (LCT); occurs at the level of the cord injury and below
- Ipsilateral diminished proprioception, vibratory sensation, and light touch: dorsal columns; occurs at the level of the cord injury and below
- Contralateral diminished pain and temperature: lateral spinothalamic tract (LST); occurs 1-2 levels distal to the cord injury and below because LST sensory neurons send axon projections up 1-2 levels prior to decussating (crossing over)
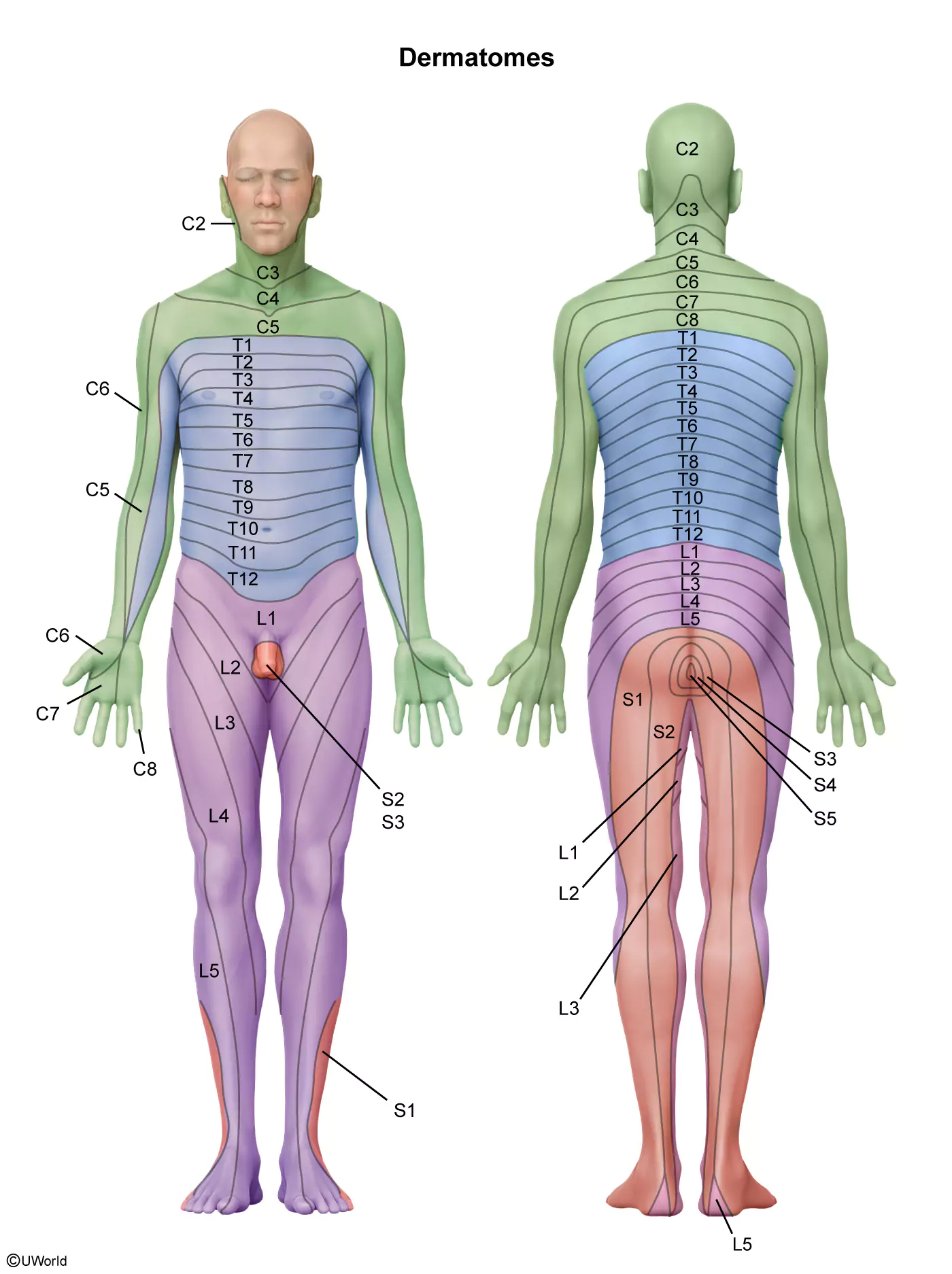
In this patient, a right spinal hemisection at T8 would cause a contralateral (left-sided) LST deficit beginning around T10 (ie, the level of the umbilicus according to the dermatomes). Such a lesion is less likely to affect contralateral pain and temperature sensation at T8 because the left-sided T8 fibers decussate to the right-sided spinal cord 1-2 levels above T8 (eg, T6, proximal to the site of injury).
{kind=link}
When Brown-Séquard syndrome occurs in the cervical region, there may be associated ipsilateral Horner syndrome (ptosis, miosis, anhidrosis). In addition, ipsilateral reflexes (including Babinski) may be initially absent due to spinal shock (ie, temporary loss of all distal spinal cord function, including spinal cord reflexes); after the spinal shock resolves, ipsilateral hyperreflexia and positive Babinski are typically present.
(Choice A) Complete spinal transection at T10 would likely cause bilateral paralysis and complete loss of sensation below the level of injury.
(Choices B, C, and E) Left spinal hemisection at T8 or T10 would cause Brown-Séquard syndrome; however, it would be opposite to this patient's presentation (eg, left leg paralysis). Right spinal hemisection at T10 would cause Brown-Séquard syndrome, but the contralateral (left-sided) LST deficit would begin around the T12 level.
Educational objective:
Hemisection of the spinal cord can cause Brown-Séquard syndrome, which is characterized by the following:
- Ipsilateral hemiparesis and diminished proprioception, vibratory sensation, and light touch at the level of the spinal cord injury and below
- Contralateral diminished pain and temperature sensation 1-2 levels distal to the cord injury and below


Try Another
Practice Question?
Log in to your FREE Trial and
keep practicing.
Upgrade
Today
Gain access to 2000+ Clinical Practice Questions for Exam Success