
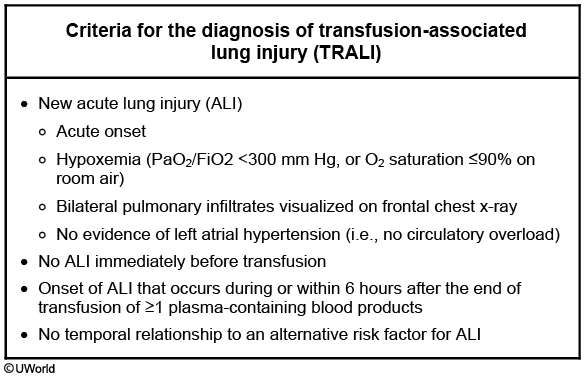
A 55-year-old man is evaluated for acute onset of respiratory distress. He was admitted to the hospital after a highway traffic accident, which resulted in a left femur and wrist fracture. He was immediately taken to the operating room and underwent open reduction and internal fixation. The total blood loss was estimated at 1.1 liters and he was given 2 liters of intravenous normal saline and one unit of packed red blood cells intraoperatively. He was extubated and transferred to the postoperative recovery room. One hour following extubation, he developed acute respiratory distress requiring reintubation. His other medical problems include inferior wall myocardial infarction with right coronary artery stent placement 3 years ago, hypertension, hyperlipidemia, and type 2 diabetes mellitus. His home medications include aspirin, metoprolol, lisinopril, metformin, and rosuvastatin.
His temperature is 38.1 C (100.6 F), blood pressure is 110/70 mm Hg, pulse is 110/min, respirations are 30/min, and oxygen saturation is 90% on 100% FiO2 and 10 mm Hg of PEEP. He is drowsy from the sedation and intravenous hydromorphone infusion. There is no jugular venous distention or lower extremity edema. Pulmonary examination reveals diffuse crackles throughout the lungs. There are no heart murmurs. Skin examination reveals no rashes.
Arterial blood gas shows a pH of 7.47, PaCO2 of 32 mm Hg, and PaO2 of 65 mm Hg.
ECG shows sinus tachycardia. His preoperative chest x-ray was within normal limits. Repeat chest x-ray taken before reintubation is shown below.

Which of the following is the most likely cause of his current condition?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A 65-year-old woman comes to the physician with a pruritic rash. This is the second year the rash has appeared, both times during the onset of winter. She has intensely pruritic areas on her lower extremities along the shins and above the right lateral malleolus. The patient sometimes experiences pruritus on her lower back and the extensor surfaces of the forearms. One area usually predominates. There is no visible rash initially, but the involved areas can become rough and scaly after a few weeks of frequent scratching. Her only other medical problem is perennial rhinitis. Her medications include cetirizine, calcium plus vitamin D supplements, and a multivitamin.
Skin examination findings are shown in the photograph.

Which of the following is the best next step in management of this patient?
{kind=link}