High Altitude Illness
Article Sections
Introduction
High altitude illness encompasses 3 conditions that develop in climbers or travelers who ascend to high altitude (generally >2500 m [8000 ft]) without sufficient time for acclimatization. They include:
- Acute mountain sickness
- High altitude cerebral edema (HACE)
- High altitude pulmonary edema (HAPE)
In addition, chronic mountain sickness, a form of pulmonary hypertension with severe polycythemia, can develop in individuals residing permanently at high altitude.
Pathogenesis
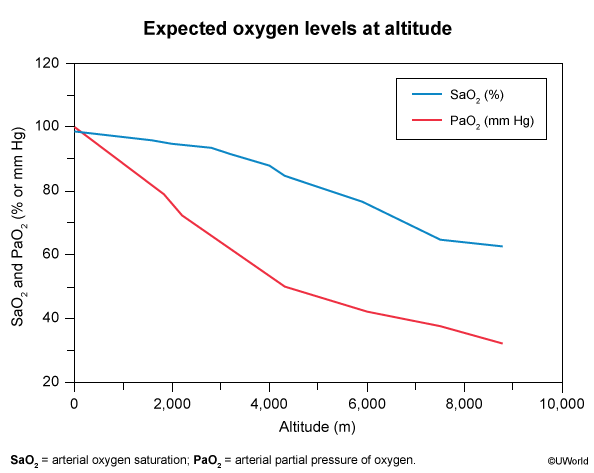
Atmospheric pressure (and therefore partial pressure of inspired oxygen [PiO2]) decreases with increasing altitude, resulting in hypobaric hypoxemia (Figure 1). Normal physiologic responses include the following (Table 1):
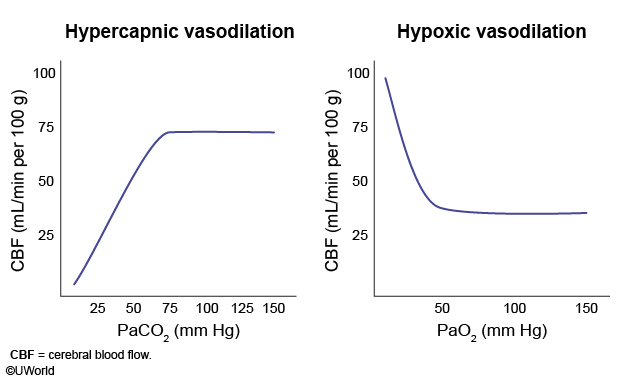
- Brain: Cerebral vasodilation results in mildly increased intracranial pressure.
- Lungs: Pulmonary vasoconstriction results in mildly increased pulmonary artery pressure. An increased ventilatory drive also causes respiratory alkalosis (↓PaCO
Continue Learning with UWorld
Get the full High Altitude Illness article plus rich visuals, real-world cases, and in-depth insights from medical experts, all available through the UWorld Medical Library.
Unlock Full AccessFigures