Nephritic Syndrome: A Comprehensive Overview
Article Sections
Introduction
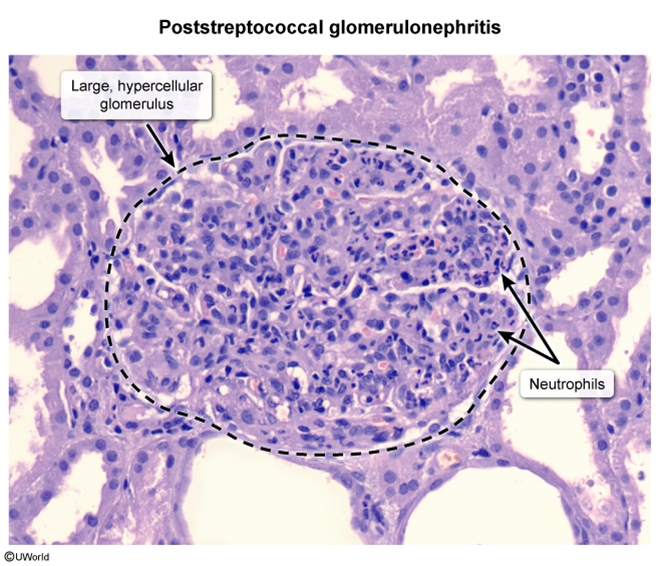
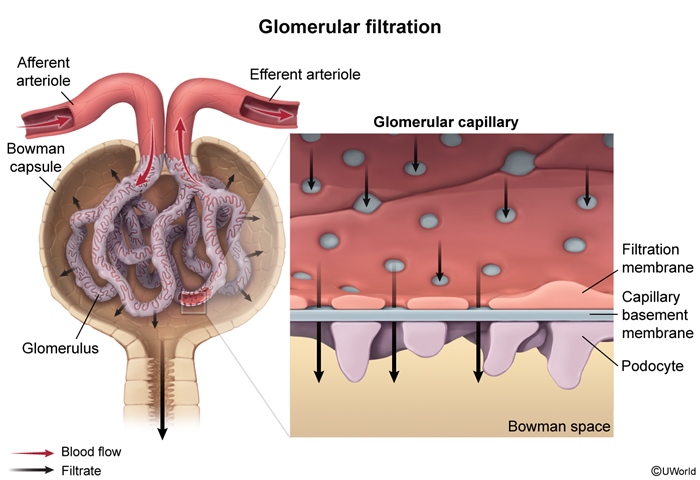
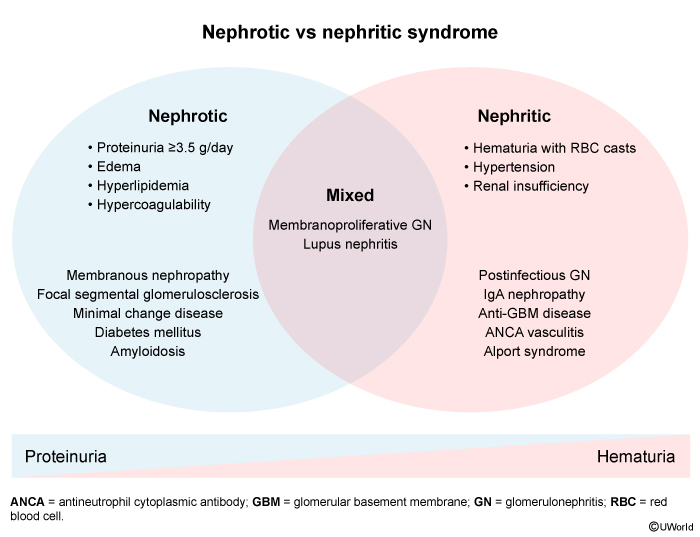
Nephritic syndrome is characterized by hematuria, hypertension, and acute kidney injury (AKI). It results from inflammation throughout the glomerulus (glomerulonephritis [GN]) involving the capillary endothelial cells, mesangial cells, and the glomerular basement membrane (GBM) (Figure 1). The hallmark of nephritic syndrome is the presence of dysmorphic red blood cells (RBCs) or RBC casts in the urine, indicating glomerular hematuria. In contrast, nephrotic syndrome involves more localized, noninflammatory injury to podocytes and the GBM that results in heavy proteinuria without glomerular hematuria (discussed in a separate article).
Pathophysiology
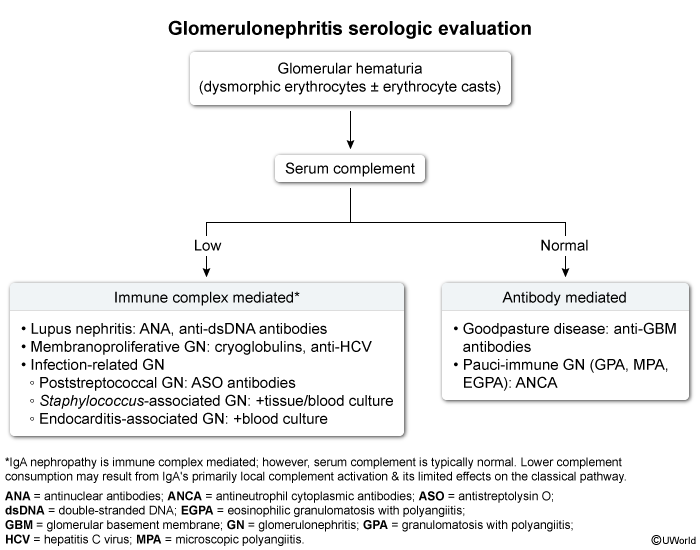
Glomerular inflammation in nephritic syndrome is typically mediated by either immune complexes or autoantibodies that target various components of the glomerulus as follows:
- Immune complex deposition: Circulating immune complexes, formed by the binding of antibodies to specific antigens, can deposit in the glomerular capillary walls or mesangium.
Continue Learning with UWorld
Get the full Nephritic Syndrome: A Comprehensive Overview article plus rich visuals, real-world cases, and in-depth insights from medical experts, all available through the UWorld Medical Library.
Unlock Full AccessFigures
Images