Herpes Zoster (Shingles)
Article Sections
Introduction
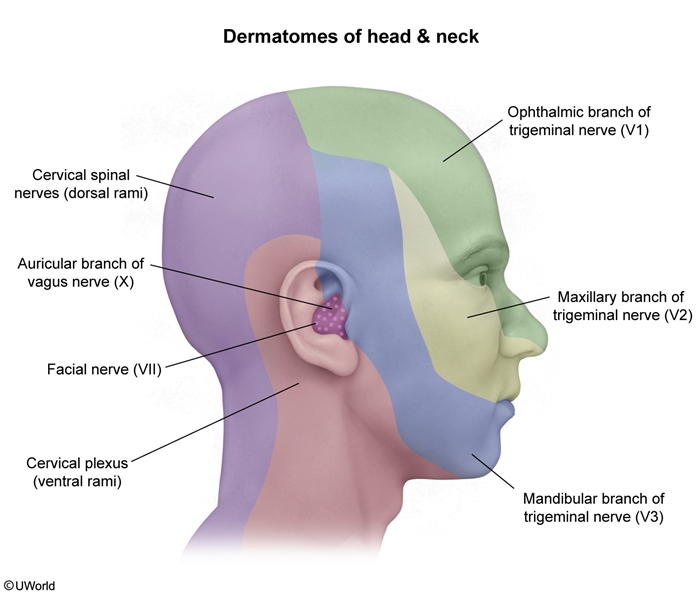
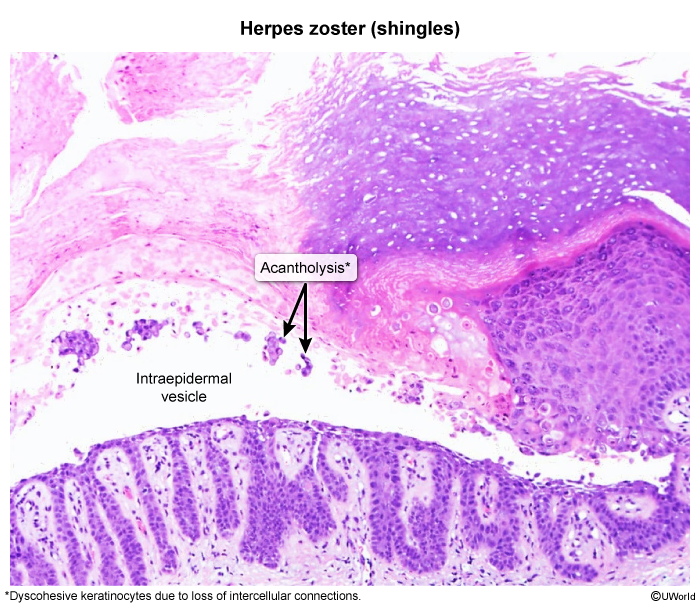
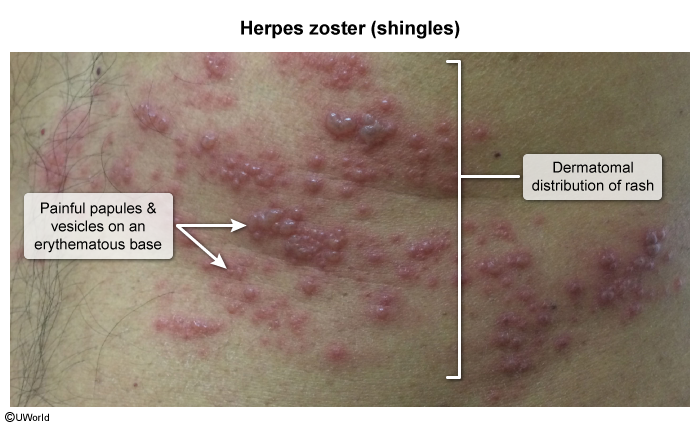
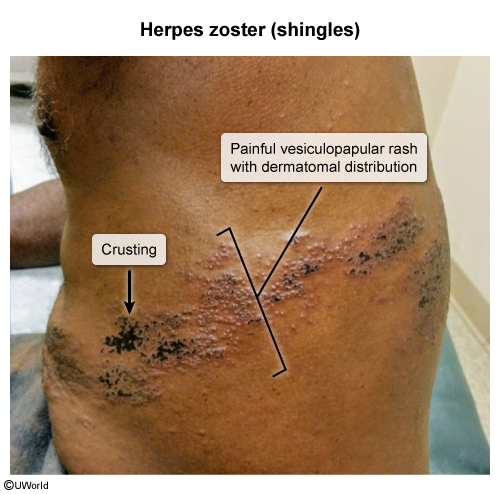
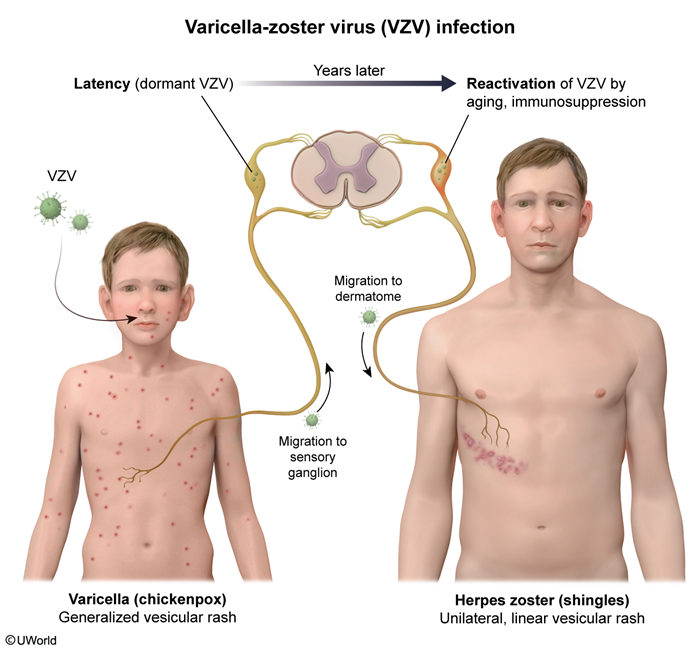
Herpes zoster (shingles) results from the reactivation of latent varicella-zoster virus (VZV), which persists in sensory ganglia after primary varicella infection (chickenpox). Its hallmark clinical presentation is a painful vesicular rash that generally occurs in a dermatomal distribution. Although usually self-limited, herpes zoster can lead to persistent neuropathic pain and sometimes present with disseminated or severe disease in immunocompromised individuals.
Pathophysiology and risk factors
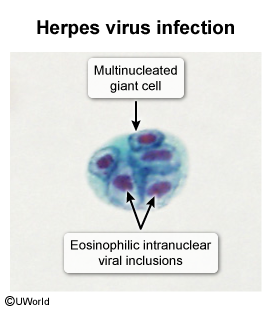
VZV, a double-stranded DNA virus of the herpesvirus family, causes the following distinct diseases:
- Primary varicella (chickenpox) infection and
- Reactivation disease (herpes zoster, or shingles).
During primary varicella infection, inoculation in the nasopharyngeal mucosa is followed by migration of the virus to the regional lymphatics. Subsequent dermatotrophic migration produces a diffuse vesicular rash (mostly located on the face and trunk) associated with fever, malaise, and pharyngitis (chickenpox). Then, the virus travels retrograde via sensory nerves to cranial nerve and dorsal spinal ganglia, where it lies dormant for decades.
Continue Learning with UWorld
Get the full Herpes Zoster (Shingles) article plus rich visuals, real-world cases, and in-depth insights from medical experts, all available through the UWorld Medical Library.
Unlock Full AccessFigures
Images