Urinary Incontinence
Article Sections
Introduction
Urinary incontinence (UI), the involuntary loss of urine, is often divided into three subtypes: stress, urgency, and overflow. The treatment and management are dependent on the predominant subtype.
Physiology
Continence (Figure 1) is normally maintained through a combination of voluntary and involuntary control.
- The cerebral cortex (upper motor neurons) maintains continence by inhibiting micturition through the pontine micturition center within the brainstem.
- The external urinary sphincter is a skeletal muscle with nicotinic receptors that receives somatic motor innervation (voluntary control) from the perineal branches of the pudendal nerve (S2-S4).
- The detrusor muscle and the internal urethral sphincter (IUS) receive autonomic innervation (involuntary control). Sympathetic stimulation (from the inferior hypogastric plexus [T11-L2] traveling through the hypogastric nerve) promotes urine storage and continence by increasing IUS tone through alpha-1 receptors and by inhibiting detrusor contractions through beta-3 agonist receptors.
Continue Learning with UWorld
Get the full Urinary Incontinence article plus rich visuals, real-world cases, and in-depth insights from medical experts, all available through the UWorld Medical Library.
Unlock Full AccessFigures
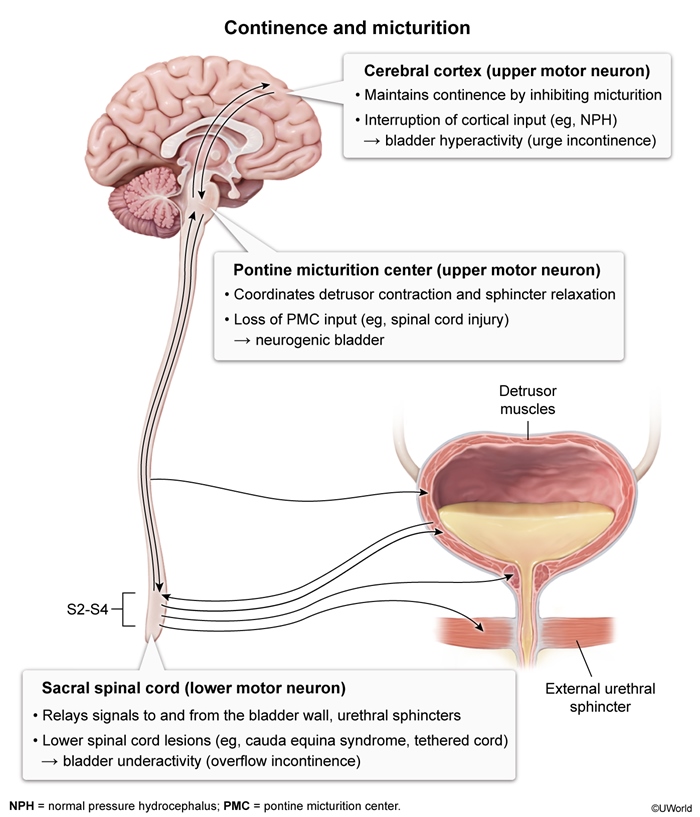
Figure 1
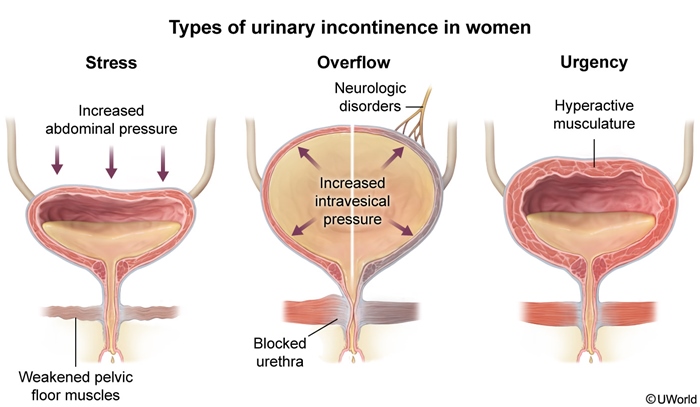
Figure 2
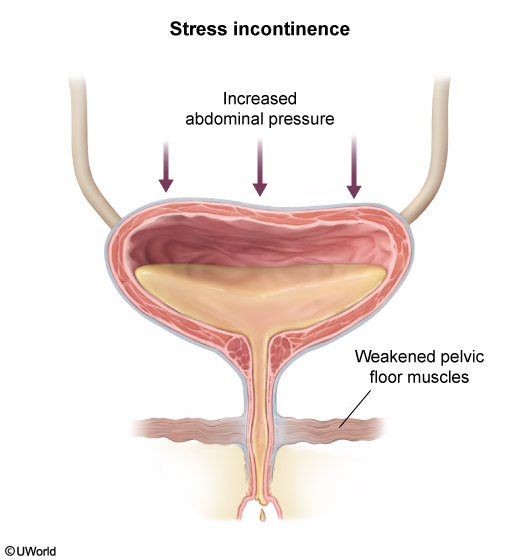
Figure 3
Figure 4
Figure 5
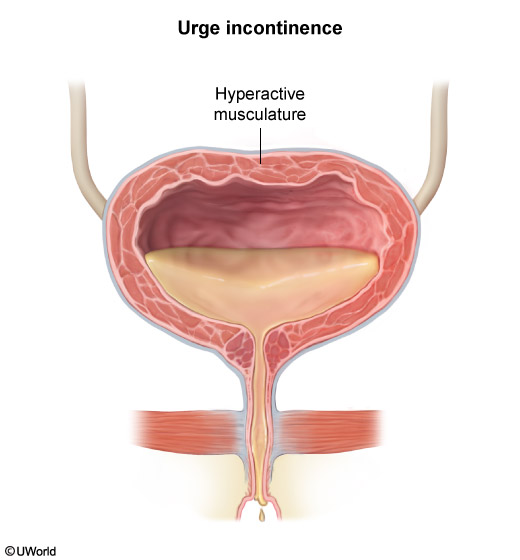
Figure 6
Medical Image
Medical Illustration